Omicron variant concerns

https://covidactnow.org/share/53615/?redirectTo=%2Fus%2Fnew_jersey-nj%2Fexplore%2F53615
In recent days the infection rate for Essex County has soared and is the highest in New Jersey! I had been feeling relatively complacent when comparing NJ to other areas reporting high infection rates and hospitalizations in recent months, that spiking is scary.

They currently do not tell you which strain is responsible.
jamie said:
When you get tested positive - do they tell you which strain it was? I think the big surprise with omicron was the rapid spread of it. Fortunately, it does sound like it is on the milder side. I can't fault any over reaction to it.


prisoners_dilemma said:
Recently had Covid. Male, mid-40's, no comorbidities. Didn't get tested until day 5 or 6 of being symptomatic, thought I had a cold. Remainder of family (including unvaxxed under 10's) didn't get anything, which was confirmed with multiple PCR tests.
That's great news, and really what is being hoped for with Omicron -- that it will lead to Covid-19 basically being like a cold going forward.
Out of curiosity, when was your most recent vax?



Our Chief Health Officer and our Health Minister here in Queensland, while talking about the rapid rise in caseloads over the next couple of weeks especially, and the subtext of how there’s little we can expect the federal government to support beyond what is already here & programmed, have highlighted some very handy resources for locals : 10 ways to protect yourself and your family from covid and other viruses, and 10 things to have in your covid toolkit.
The first one isn’t practical for you at this time of year  However, I’m not sure if anyone has suggested MOLers and their neighbours should prepare Toolkits, or Go-Bags. As Dr Gerard said, we prepare them anyway for fire/flood/cyclone season, these ones are tailored for covid. https://www.qld.gov.au/__data/assets/pdf_file/0016/230605/covid-ready-kit.pdf Very smart idea that helps you feel a little more in control of your destiny.
However, I’m not sure if anyone has suggested MOLers and their neighbours should prepare Toolkits, or Go-Bags. As Dr Gerard said, we prepare them anyway for fire/flood/cyclone season, these ones are tailored for covid. https://www.qld.gov.au/__data/assets/pdf_file/0016/230605/covid-ready-kit.pdf Very smart idea that helps you feel a little more in control of your destiny.
Do remember the phone numbers in that document are Australian! Replace them with local resources!
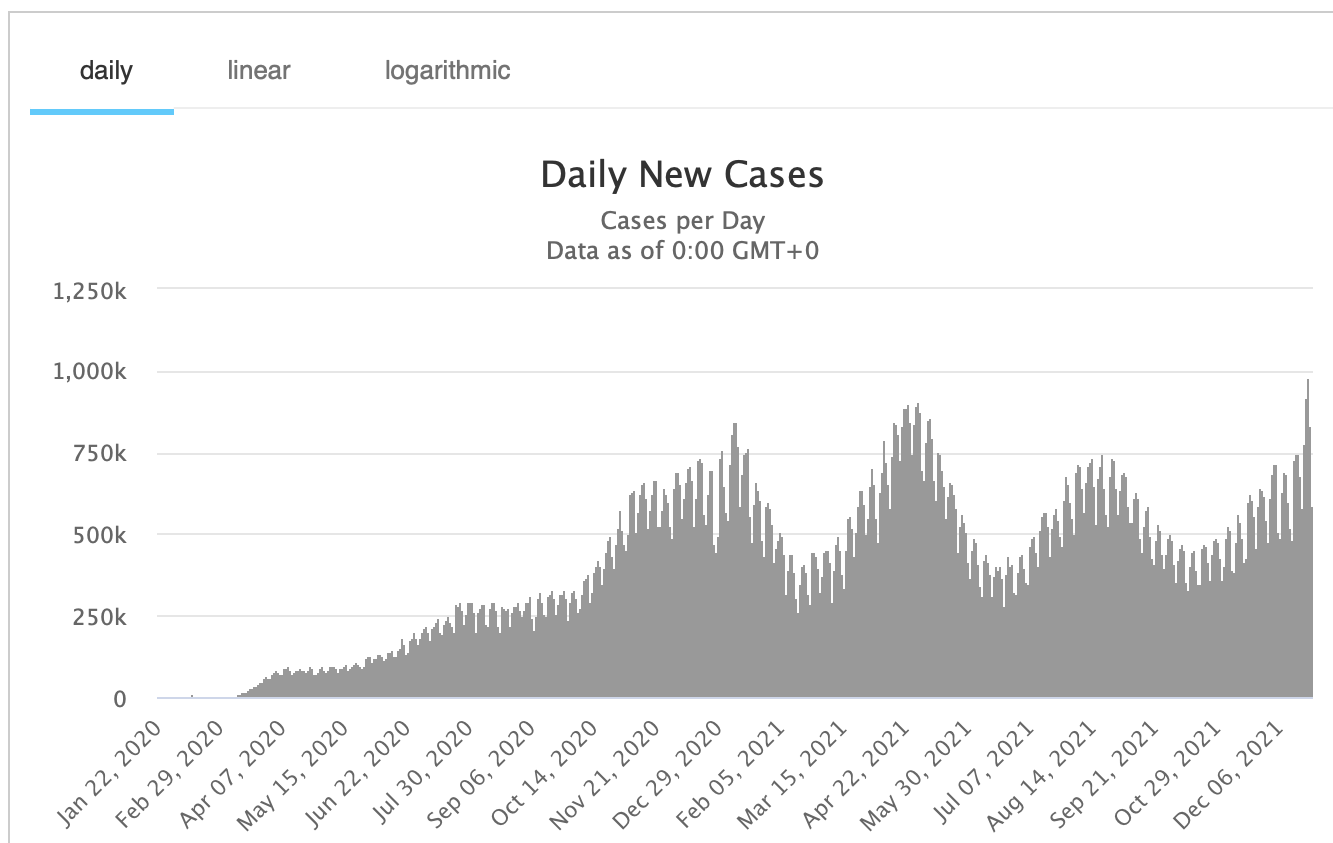
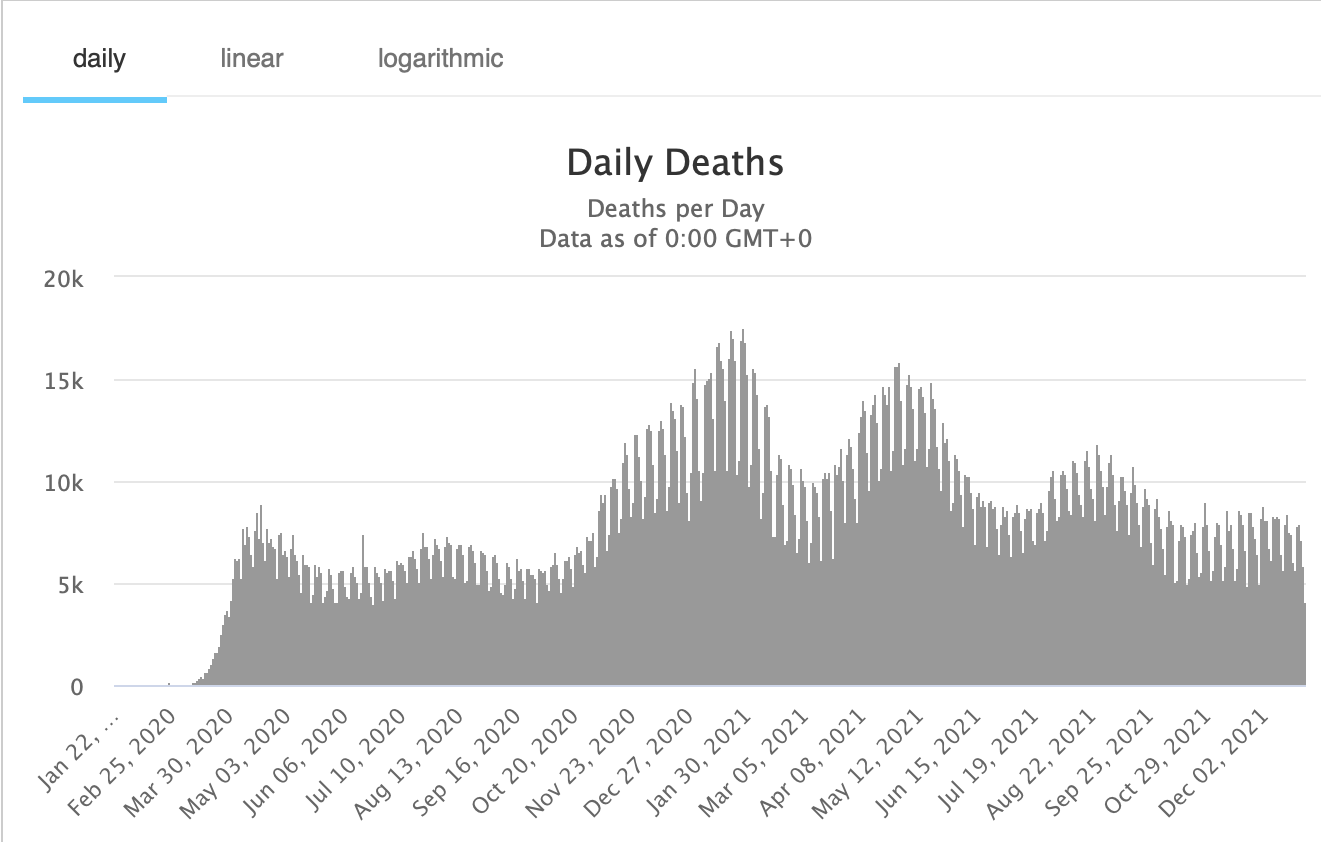
The infection rates we're seeing with this variant are stunning but we've also heard about how it doesn't cause illness that gets as bad as that from the prior versions of COVID-19.
TL-DR: This report shreds light on why omicron infects people so readily but can't do as much damage because the mutations muck up its ability to fully invade the cells it attaches to.
This is a report on some research that uses a neat technique to study how mutations affect the spike protein. It isn't peer-reviewed yet and it's only in the lab but it's just plain cool - if you're as geeky about this stuff as I am. They have a way of observing the activity of the spike protein versions in a system that is very close to how it works in the live virus - how it latches onto and invades its target cells so it can do its thing on the inside. But this experimental model doesn't have the rest of the virus with it. One way to think of it would be like a way to tweak the fob for one of the new cars that doesn't use one of those keys we used to have to plug into the starter.
If some tweak (to simulate a mutation) lets it open the door, aha! We've learned something but we don't have to worry about it being able to sit in the driver's seat and start it up by pushing the button. Ehh, this analogy needs some work.
https://www.livescience.com/omicron-less-severe-disease-early-evidence

jamie said:
When you get tested positive - do they tell you which strain it was? I think the big surprise with omicron was the rapid spread of it. Fortunately, it does sound like it is on the milder side. I can't fault any over reaction to it.
they don’t tell you

Parkway today. Stopped at two rest stops. 100% masked. About 30 people, total.

Local good news re the seeming mildness of Omicron, at least for the vaccinated. On the one hand, there has been a very dramatic spike in positive tests in the towns around here despite high vaccination rates (there is an Essex County site where you can see the daily numbers for each town) . Yet I'm an EMT and I've noticed no spike in 911 calls that are definitely or suspected to be Covid related. I can't remember the last time I saw a 911 dispatch that said "positive for Covid." The absence of a spike in 911 calls makes sense to me because If you take "difficulty breathing" out of the equation - which seems to correspond to to the findings that Omicron does not attack the lungs very effectively - it's hard to see how other symptoms would drive people to the hospital. You'd have to have one scary headache, or sore throat, or body ache to make you think "I better go to the hospital."
To be clear, I'm not encouraging any kind of laxness. Get vaccinated, get boosted , wear good masks, avoid unnecessary indoor gatherings etc. We still want to slow this down. Statewide, hospitalizations and ventilator use has ticked up significantly with the spread of Omicron.

While Omicron increases optimism about avoiding hospitalization, I'm also worried about "long covid" PASC, which I'm guessing is affecting over 7 million+ people in the US, based on the 50 million that have been infected here, and could last years if not for life:
https://www.webmd.com/lung/what-is-long-covid-pasc#1
"Research shows that about 10% of people between ages 18 to 49 who have COVID-19 get long COVID. The odds go up to 22% for those 70 or older. But it can happen to anyone, whether you’re otherwise healthy or have other health conditions. You can get it even if your earlier COVID-19 symptoms were mild or moderate........Long COVID appears to affect each person in different ways. You might notice a wide range of things that could linger for a long time. Common symptoms include:
"Fatigue. Brain fog. Loss of smell and taste. Shortness of breath. Cough. Joint pain. Chest pain. Sleep issues. .Anxiety. Gut problems. Fever. Muscle pain. Depression. Headache. Rapid heartbeat. ......In rare cases, long COVID can affect your organs. You may get: Inflammation of your heart muscle. Lung-related issues. Kidney problems. Hair loss. Skin rashes. A hard time with concentration and memory."


bub said:
Local good news re the seeming mildness of Omicron, at least for the vaccinated. On the one hand, there has been a very dramatic spike in positive tests in the towns around here despite high vaccination rates (there is an Essex County site where you can see the daily numbers for each town) . Yet I'm an EMT and I've noticed no spike in 911 calls that are definitely or suspected to be Covid related. I can't remember the last time I saw a 911 dispatch that said "positive for Covid." The absence of a spike in 911 calls makes sense to me because If you take "difficulty breathing" out of the equation - which seems to correspond to to the findings that Omicron does not attack the lungs very effectively - it's hard to see how other symptoms would drive people to the hospital. You'd have to have one scary headache, or sore throat, or body ache to make you think "I better go to the hospital."
To be clear, I'm not encouraging any kind of laxness. Get vaccinated, get boosted , wear good masks, avoid unnecessary indoor gatherings etc. We still want to slow this down. Statewide, hospitalizations and ventilator use has ticked up significantly with the spread of Omicron.
I would suggest another factor — people know the seriousness and the symptoms, and are being taken to the hospital a bit earlier in the infection if needed (as one local mom did with a 1.5 year old with COVID and high fever). We also are only a week or two into the major wave, so haven’t seen many patients in week two or three, when complications may be more likely to arise.
Jasmo, I share your concern about long haul COVID. I have a cousin who is a gig worker, significant risk factors (cancer survivor with well controlled diabetes), fully vaccinated, and got a breakthrough case a few months ago that put him in the hospital and left him with long-haul symptoms. He is burning through his savings while trying to get healthy enough to work a few more years before retirement.

I spoke this morning with a charge nurse at a local hospital. She told me the number of their COVID hospitalizations, primarily of the unvaccinated, has increased to the point where the hospital has started to turn away elective surgeries that would require a hospital bed for recovery. She also stated that number of pediatric COVID admissions is on the rise to the point where a separate COVID ward has been created for these patients. The impact on the health care system at her hospital is real and expected to get worse. She does not suspect a return to March 2020 numbers of COVID hospitalizations for a lot of reasons: vaccination availability, better treatment protocols, contract tracing, etc. Still, she cautions that wer have to treat the presence of the Omicron variant very seriously.
sprout said:
That's great news, and really what is being hoped for with Omicron -- that it will lead to Covid-19 basically being like a cold going forward.
Out of curiosity, when was your most recent vax?
I got jabbed in April with the J&J shot, so highly likely that my immunity had waned significantly.

With this many cases, one has to wonder what sort of new variants are down the road. Omicron happened to be less severe but the next one could easily be both more transmissible AND more severe. Every additional case is an opportunity for the virus to mutate.
PeterWick said:
These data suggest otherwise but I'm very glad your experience was essentially uneventful. The link below will come off as fear porn to you from what I gather but I have to say that your claim of ">99.50%" is unwarranted.
https://www.cnn.com/2021/12/22/health/2020-death-data-cdc/index.htmlIn the link below are worldwide data. The 5.3M deaths out of 272.5M cases comes to just under 2%.
https://fullfact.org/health/Covid-recovery-vaccine/
And "not dead" does not mean fully recovered. Statistics on the consequential morbidities after recovering from COVID are harder to come by but this Mayo Clinic link provides some information. COVID infections cause bodily events that are not easily healed such as blood clots and the damage they can cause wherever they wind up stuck in the body's blood vessels. That's just one scenario and there are many other lasting conditions that still have yet to be understood.
https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-long-term-effects/art-20490351
Article from the Imperial College suggests IFR's in low income countries is about 0.23% while in high countries is 1.15%.
https://www.imperial.ac.uk/news/207273/covid-19-deaths-infection-fatality-ratio-about/
A bulletin from the WHO by John Ioannidis IFR based on seroprevalence data: the median IFR was 0.27% corrected to 0.23% across 51 locations. His conclusion was that "The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic."

I don't think that unvaccinated Covid patients (who are eligible for the vaccine) should be admitted if it will take beds away from non-Covid or vaccinated Covid patients who need them, including so-called elective surgery/treatment patients whose conditions might worsen if treatment is delayed. JMHO
sac said:
I don't think that unvaccinated Covid patients (who are eligible for the vaccine) should be admitted if it will take beds away from non-Covid or vaccinated Covid patients who need them, including so-called elective surgery/treatment patients whose conditions might worsen if treatment is delayed. JMHO
Tempting, but a dangerous road to travel. Do we also put smokers at the back of the line for hospital care? Drug users? People who had accidents because they were speeding? Unhelmeted motorcyclists? People with BMIs above certain limits? Shifting from disease based triage to lifestyle judgment triage seems problematic to me (and only encourages the use of fake vaccine cards).
prisoners_dilemma said:
PeterWick said:
These data suggest otherwise but I'm very glad your experience was essentially uneventful. The link below will come off as fear porn to you from what I gather but I have to say that your claim of ">99.50%" is unwarranted.
https://www.cnn.com/2021/12/22/health/2020-death-data-cdc/index.htmlIn the link below are worldwide data. The 5.3M deaths out of 272.5M cases comes to just under 2%.
https://fullfact.org/health/Covid-recovery-vaccine/
And "not dead" does not mean fully recovered. Statistics on the consequential morbidities after recovering from COVID are harder to come by but this Mayo Clinic link provides some information. COVID infections cause bodily events that are not easily healed such as blood clots and the damage they can cause wherever they wind up stuck in the body's blood vessels. That's just one scenario and there are many other lasting conditions that still have yet to be understood.
https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-long-term-effects/art-20490351Article from the Imperial College suggests IFR's in low income countries is about 0.23% while in high countries is 1.15%.
https://www.imperial.ac.uk/news/207273/covid-19-deaths-infection-fatality-ratio-about/
A bulletin from the WHO by John Ioannidis IFR based on seroprevalence data: the median IFR was 0.27% corrected to 0.23% across 51 locations. His conclusion was that "The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic."
The data discussed in each of those two articles only comes from October 2020 at the latest. The FullFact.org link I cited is also from the fall of 2020 and it has a different interpretation. That time frame also does not include the three substantial surges in daily cases and daily deaths starting in the winter of 2020 on into the late summer of 2021. The prevalence of the delta variant made some changes to the IFR that they do not account for. Today's Worldometer stats show 5.4M deaths out of 280.33M cases which comes to a greater than 1.9% IFR.
Hardly a nothing burger. Plus, we've seen more evidence of the ways "long haul" COVID survivors are affected by this infection.
https://www.ama-assn.org/delivering-care/public-health/what-doctors-wish-patients-knew-about-long-covid
This is a report from October 2021 on the rate at which COVID survivors experience continued problems from one or more of an array of symptoms.
https://www.forbes.com/sites/marisadellatto/2021/10/13/more-than-half-of-covid-19-patients-suffer-from-long-haul-symptoms-study-finds/?sh=673423b7f91b
sac said:
I don't think that unvaccinated Covid patients (who are eligible for the vaccine) should be admitted if it will take beds away from non-Covid or vaccinated Covid patients who need them, including so-called elective surgery/treatment patients whose conditions might worsen if treatment is delayed. JMHO
I can see how this feeling really burns in peoples' minds but as susan1014 says, there are many other situations where society hasn't closed the door on medical care for conditions that could have been prevented or at least the risks reduced. Unfortunately, getting overwhelmed with COVID patients can seem like a field hospital after an armed battle where triage is a hard discipline to live with.

PeterWick said:
The data discussed in each of those two articles only comes from October 2020 at the latest.
At dinner tonight my family was discussing the hazards of relying on secondary sources of information (in general; not just about Covid). That led to agreement that primary sources can be trouble, too, if we don’t know how to handle them.
You know, whether any variant is experienced as mild or not by one individual or another, or someone else is struggling to find a bed in hospital doesn’t really matter overall to me. What matters most is that here we have major labs so overwhelmed that already just under 1500 people have been notified that their results were Negative for covid when in fact they’re Positive and over 2/3 are omicron.
If it’s happening in Australia with our relatively small caseloads compared with USA, I feel sorry for your contract tracers and lab workers.
susan1014 said:
Tempting, but a dangerous road to travel. Do we also put smokers at the back of the line for hospital care? Drug users? People who had accidents because they were speeding? Unhelmeted motorcyclists? People with BMIs above certain limits? Shifting from disease based triage to lifestyle judgment triage seems problematic to me (and only encourages the use of fake vaccine cards).
All on the list except B.M.I. are voluntary choices. If triage is based on lack of resources, leave their **** out on the curb.
Oh,
We already do triage treatment. Try to get a liver transplant if you are an alcoholic.
Medical, life insurance and automobile rates are often based upon prior lifestyle choices and history. Perhaps those choosing not to get vaxxed should be required to pay more insurance based upon probable medical needs and actuarial tables.
Formerlyjerseyjack said:
susan1014 said:
Tempting, but a dangerous road to travel. Do we also put smokers at the back of the line for hospital care? Drug users? People who had accidents because they were speeding? Unhelmeted motorcyclists? People with BMIs above certain limits? Shifting from disease based triage to lifestyle judgment triage seems problematic to me (and only encourages the use of fake vaccine cards).
All on the list except B.M.I. are voluntary choices. If triage is based on lack of resources, leave their **** out on the curb.
Oh,
We already do triage treatment. Try to get a liver transplant if you are an alcoholic.
Formerlyjerseyjack said:
We already do triage treatment. Try to get a liver transplant if you are an alcoholic.
That sounds like an example of what Peter referred to as disease-based triage, because of the potential of alcoholism to damage the transplanted liver. (Also, while there’s ongoing debate, alcoholics do get liver transplants, from what I’ve read.)
DaveSchmidt said:
Formerlyjerseyjack said:
We already do triage treatment. Try to get a liver transplant if you are an alcoholic.
That sounds like an example of what Peter referred to as disease-based triage, because of the potential of alcoholism to damage the transplanted liver. (Also, while there’s ongoing debate, alcoholics do get liver transplants, from what I’ve read.)
Yes, medical triage generally depends on medical factors (prioritizing the most serious of those who are likely to be saved) rather than moral judgments. Having higher insurance premiums for lifestyle choices is a standard thing that might be applied to COVID, although it comes with the very real risk of more people choosing to go uninsured and thus becoming greater burdens on the general public (via governments and hospitals).
Question: If you are fully vaccinated, but had a breakthrough infection over a months ago, and live in NYC, and are planning on foreign travel this week and must be tested within 72 hours of travel; then should you get a rapid antigen or PCR test? The concern is that the nasal PCR test may show a false positive from the prior infection from over a month ago? The person has fully recovered and has no symptoms. In reading over the CDC and other info, It seems that the rapid antigen test is the best choice and especially due to the need for a rapid test and the difficulty of long lines to get a test.
PS, this is my son who has had this trip planned for many months. While the delay of the trip may be an option, it is not preferred for multiple good reasons.
susan1014 said:
DaveSchmidt said:
Formerlyjerseyjack said:
We already do triage treatment. Try to get a liver transplant if you are an alcoholic.
That sounds like an example of what Peter referred to as disease-based triage, because of the potential of alcoholism to damage the transplanted liver. (Also, while there’s ongoing debate, alcoholics do get liver transplants, from what I’ve read.)
Yes, medical triage generally depends on medical factors (prioritizing the most serious of those who are likely to be saved) rather than moral judgments. Having higher insurance premiums for lifestyle choices is a standard thing that might be applied to COVID, although it comes with the very real risk of more people choosing to go uninsured and thus becoming greater burdens on the general public (via governments and hospitals).
Denying liver for alcoholics is also moral. Who is anyone to assume the life style choice or need of an alcoholic in need of a transplant will continue to be alcoholic? The shock of needing a liver may "cure' the patient.
COVID triaging leading to denial of the unvaccinated is not just a moral issue. Its also medical. Many unvaccinated COVID patients will still refuse vaccination. Like an alcoholic needing a liver and possibly continue being a high risk, we have the unvaccinated needing treatment who also continue being high risk.
These issues seem to me both medical and moral.
But I would prioritize. If you need liver and there is a shortage then give it to the non-alcoholic. If you need COVID treatment and there is a shortage of beds give it to the vaccinated.
RTrent said:
COVID triaging leading to denial of the unvaccinated is not just a moral issue. Its also medical. Many unvaccinated COVID patients will still refuse vaccination.
Medical personnel who make triage decisions are presumably aware of the natural immunity that will exist whether or not the Covid survivor gets a vaccination.

Sponsored Business





Promote your business here - Businesses get highlighted throughout the site and you can add a deal.







Harrowing article from the Guardian. Among other things it describes a "mild" breakthrough infection in a vaccinated, boosted ER nurse:
On her fourth day of Covid symptoms, Ruth woke up in the worst pain of her life. It felt like her joints were filled with broken glass; she couldn’t walk, couldn’t move. “It was worse than childbirth,” she said.
When friends texted to check on her, she couldn’t hold the phone or move her fingers to write back. Her doctor called in medication, and it took Ruth 40 minutes to shuffle to the pharmacy half a block away.
But the main points are a) nursing shortage and b) overwhelmed hospitals.
https://www.theguardian.com/us-news/2021/dec/23/us-hospitals-staffing-shortages-omicron-covid