Omicron BA.2 wave may be causing a wave that is hard to quantify




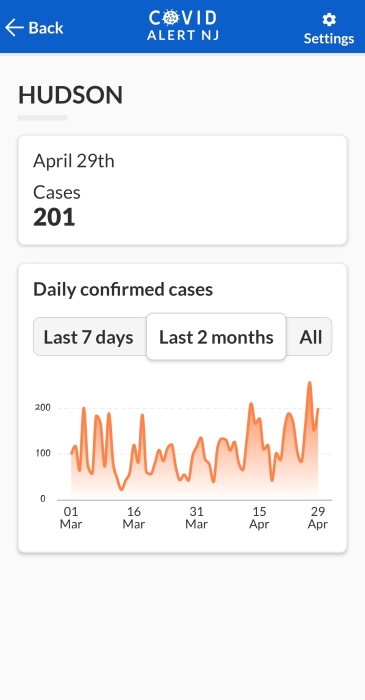

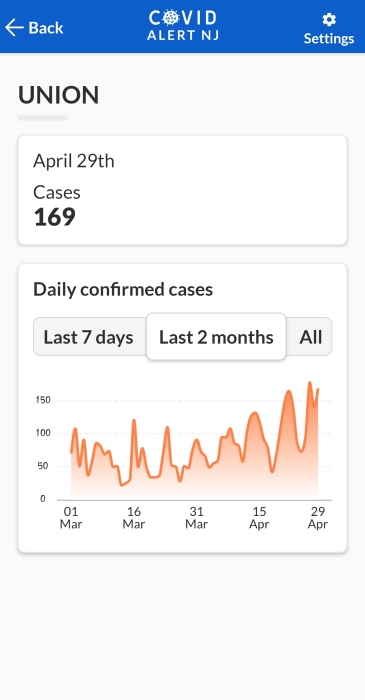

Those numbers aren't anywhere near what happened when the first omicron wave came upon us in December 2021 but it's a steady increase.
Hospitalization rates haven't shot up but there is much greater recognition of the growing numbers of long COVID patients.
You don't want to get COVID at all if you can help it.

There is a lot of information in this article about long COVID
https://health.ucdavis.edu/coronavirus/covid-19-information/covid-19-long-haulers
About 20-30% of children who get COVID-19 will have long COVID, which is a little less than half the rate that adults experience lasting symptoms. Vaccines are shown to prevent long COVID. Since they help prevent COVID-19 infection, they also protect about 90% against getting long COVID.
However, even children who have no COVID-19 symptoms but test positive for the virus can have long COVID. That's why it's important to prevent all cases, even those where children are asymptomatic. Pediatricians encourage parents to get their children vaccinated if they're eligible. The next best protection is to wear a mask.
Pediatric hepatitis - a rare condition in the U.S. - outbreaks are now occurring around the world and the cause is unclear but many of the usual causes of it have been ruled out. Adenovirus is
https://www.cdc.gov/media/releases/2022/s0421-hepatitis-alert.html
This uncertainty has been mocked by some saying it's caused by the Idunnovirus but there is also a contingent blaming it on the COVID vaccines.
https://www.newsweek.com/fact-check-are-child-hepatitis-cases-linked-covid-19-vaccines-1701138
The UKHSA said none of the confirmed cases in under 10s were vaccinated, stating: "There is no link to the coronavirus (COVID-19) vaccine." WHO has also said the vast majority of affected children have not been vaccinated.
https://pubmed.ncbi.nlm.nih.gov/35149651/
Severe Hepatitis in Pediatric COVID-19
The abstract from that link:
Hepatic involvement in COVID-19 is typically characterized as mild hepatitis with preserved synthetic function in children. Severe hepatitis is a rare complication of COVID-19 infection that has not been extensively described in the pediatric population. We report a case series of 4 previously healthy children who presented with significant hepatitis as the primary manifestation of COVID-19 infection. Two of these patients met criteria for acute liver failure. None of the patients had respiratory symptoms. One patient was found to have complement dysfunction resulting in microangiopathic features and was treated successfully with eculizumab. This case is in line with adult post-mortem data showing that more severe cases of hepatic dysfunction secondary to COVID-19 infection may be associated with complement activation and microangiopathic features. Liver function should be evaluated in cases of severe COVID-19, and SARS-CoV-2 infection should be considered as a cause of acute severe hepatitis even in patients without significant respiratory or other systemic symptoms.

I think I read recently that antibody testing can now differentiate if you have had a covid infection and have also been vaccinated. The covid infection antibody is different from the vaccine antibody. Is this accurate? If it is, then we will be able to get a lot more info on the total number of covid infections. It will also be helpful in determining possible side effects from the infection vs. side effects from the vaccine. There is so much to learn.
Covid has been a tricky medically challenging virus and its illness manifestations in our bodies come in many different ways and can affect several organ systems, not just respiratory or fever-type symptoms.

Anecdotally, people I know have gotten fast moving cold-like cases, self-testing and I guess not otherwise reporting (but not sure under-reporting was dramatically different during Omicorn1). But the serious numbers don't lie. Hospital numbers have not shot up to anything like they were during Omicron and the vent numbers are as low as they have ever been during the whole pandemic. Considering how care free people have been in recent months and how the rules have relaxed, I'm cautiously optimistic that we are in a better place notwithstanding the recent rise in cases.
There was just an article that said 58% of people tested positive for actual antibodies recently, double the amount before the last wave.
bub said:
Hospital numbers have not shot up to anything like they were during Omicron and the vent numbers are as low as they have ever been during the whole pandemic. Considering how care free people have been in recent months and how the rules have relaxed, I'm cautiously optimistic that we are in a better place notwithstanding the recent rise in cases.
Acute case loads in hospitals and vent usage remain low. That is encouraging, yes.
But there is a growing concern over the huge number of COVID survivors who have been reporting lingering symptoms. Over 10% of survivors, all ages and all different severities, have what is referred to as long COVID. The symptoms of which have much in common with ME and CFS as well as brain injuries, particularly in how they report others do not believe them.

COVID PTSD is being diagnosed now as well. Should help some with monetary relief for those unable to return to work due to the pandemic through disability.
the18thletter said:
COVID PTSD is being diagnosed now as well. Should help some with monetary relief for those unable to return to work due to the pandemic through disability.
I would hope so but from what I know in the brain injury community, SS Disability grants are not given out easily. Strokes, brain cancer, TBI, anoxic injuries, encephalitis - it is almost as if they look for reasons to judge the applicant not eligible. Now we're going to have a large wave of people applying due to COVID sequelae of some sort. We'll see how well they're believed.
I don't know what to make of the long Covid situation. I know you've posted a lot of reports about it. Like everyone I suppose, I know and know of a lot of people who have had one version or another of it going back to the beginning. In my anecdotal universe, I've heard about one maybe two people who have had long Covid issues. Nobody I actually know, or their kids or spouses, have had LC. It's possible there are latent problems but as far as symptomatic long Covid, I just haven't heard of it from friends, relatives colleagues, neighbors etc.
bub said:
It's possible there are latent problems but as far as symptomatic long Covid, I just haven't heard of it from friends, relatives colleagues, neighbors etc.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00299-6/fulltext

I assume people are reporting Covid cases to the schools when they test positive on the at-home tests. So, it's possible that the school COVID dashboard is a good hyper-local measure of cases:
https://www.somsd.k12.nj.us/coviddata/
It was lower in Feb/early March. Since then, cases have been hovering around upper 20's and into the 30's each week.
sprout said:
I assume people are reporting Covid cases to the schools when they test positive on the at-home tests. So, it's possible that the school COVID dashboard is a good hyper-local measure of cases:
https://www.somsd.k12.nj.us/coviddata/
It was lower in Feb/early March. Since then, cases have been hovering around upper 20's and into the 30's each week.
No, because only PCR verified cases go on the Dashboard, as I understand it. Home test results are being accepted for unlocking remote learning, I’m told, leaving less incentive to take kids for formal testing.

Just a note to the MOL community. Peter is not a licensed doctor or scientist. Not an expert.
Peter - Stop playing the expert. Stop trying to scare people unnecessarily.
PeterWick said:
I would hope so but from what I know in the brain injury community, SS Disability grants are not given out easily. Strokes, brain cancer, TBI, anoxic injuries, encephalitis - it is almost as if they look for reasons to judge the applicant not eligible. Now we're going to have a large wave of people applying due to COVID sequelae of some sort. We'll see how well they're believed.
For those of you who have had lingering symptoms post-COVID, referred to as long COVID, or post-acute sequelae of SARS-CoV-2 infection (PASC) in some scientific journals, this is a long but interesting comparison between neuro-PASC and myalgic encephalomyelitis (ME)/chronic fatigue syndrome (CFS).
Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome
https://www.cell.com/trends/molecular-medicine/fulltext/S1471-4914(21)00134-9?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS1471491421001349%3Fshowall%3Dtrue
Lingering symptoms after acute COVID-19 may be due in some patients to chronic damage to the lungs, heart, and kidneys, and in other patients, they may be due to the psychosocial trauma of the illness and the impact of the pandemic on family, friends, and the workplace. In other patients without evidence of such chronic organ damage, such as those with post–COVID-19 syndrome, it seems likely that the underlying biology is similar to that of other postinfectious fatigue syndromes, to post–critical illness syndrome, and to that of ME/CFS. It also is likely that the underlying pathology involves the CNS; the autonomic nervous system; and a persistent, dysregulated immune and metabolic response to any of multiple infectious agents.
The COVID-19 pandemic is likely to greatly increase the number of people who develop ME/CFS or a similar illness and other post-COVID illnesses (e.g., chronic hypoxia from impaired lung function, congestive heart failure from post-COVID cardiomyopathy) [88.]. Before the pandemic, ME/CFS was estimated to impact 836 000 to 2.5 million Americans and to cost as much as $24 billion annually [89.]. An estimated 10 million people may be affected worldwide [88.]. It is too early to know the ultimate health impact of post-COVID chronic illnesses; however, senior economists have estimated that the cumulative future costs in the USA may be as high as $4.2 trillion [90.].
This new population of patients has been subject to the kind of dismissive treatment ME/CFS sufferers have gotten to know all too well.
This is an interesting paragraph way down the page, just before the references:
Will abnormalities that distinguish people with ME/CFS and post–COVID-19 syndrome at baseline become worse after physical, cognitive, and emotional stressors that typically worsen symptoms and thereby suggest that they may be directly connected to the disease process that generates the symptoms?
algebra2 said:
Just a note to the MOL community. Peter is not a licensed doctor or scientist. Not an expert.
Peter - Stop playing the expert. Stop trying to scare people unnecessarily.PeterWick said:
I would hope so but from what I know in the brain injury community, SS Disability grants are not given out easily. Strokes, brain cancer, TBI, anoxic injuries, encephalitis - it is almost as if they look for reasons to judge the applicant not eligible. Now we're going to have a large wave of people applying due to COVID sequelae of some sort. We'll see how well they're believed.
Peter has a PhD in Pharmacology. He may not be a covid expert but he is definitely a scientist. He certainly knows his way around biomedical research and scientific literature. He's a terrific resource for MOL. I've asked him for medical and scientific guidance several times over the years and always found his suggestions helpful.
If you're questioning his comment about getting disability, I can confirm that it's shockingly difficult to get SSDI. The long-COVID patients will be homeless before they see a dime.

Is it still the BA2 going around? It seems pretty mild at least. Just interesting to see who has been getting it lately. Kimmel, Colbert, Harris and now Gates!

A bunch of my friends in the UK have caught it in recent weeks, and a good friend of mine in south Jersey just tested positive, too. Cases are rising locally, but not panic-worthy according to Gov. Murphy. Of course, it's still best to avoid it, considering the after-effects, so I'm still masking in major public places.
The hospitalization # is about 700. Historically the bottom of the wave was about 500-700. They think the actual number of cases world wide is 70-90% higher than the number reported...but the hospitalizations are remaining low in NJ. They are guessing 1 in 3 people will pick it up over the winter due to losing immunity and new variants.

it appears the best advice is to get another vaccination if your last was more than six months ago.
ml1 said:
it appears the best advice is to get another vaccination if your last was more than six months ago.
And to self-protect with masking when you're indoors.
ridski said:
Cases are rising locally, but not panic-worthy according to Gov. Murphy. Of course, it's still best to avoid it, considering the after-effects, so I'm still masking in major public places.
Relying on the hospitalization or ICU bed occupancy rates may not be as valuable as it may have been with earlier waves. I've held off on posting many journal articles referring to the growing number of cases and recognized causes of long COVID sequela or PASC. Those problems usually do not send a person to inpatient treatment. They're most handled on an outpatient basis. Notice I didn't say "treated" since it is very hard to determine how these symptoms happen and are sticking around. Yes, it is after recovering from a COVID infection(s), but just what exactly is going on once the virus has supposedly left?
SO PLEASE! CONTINUE TO PROTECT YOURSELF WITH A MASK. YOU DO NOT WANT ANY OF THIS.
Until they have good evidence to explain the various symptoms, treating them is difficult. Gaslighting those patients and dismissing their concerns is pretty easy though. At least they have that down.

Rentals

Sponsored Business

Promote your business here - Businesses get highlighted throughout the site and you can add a deal.
Advertisement

This article from The Atlantic discusses the possibility but it is hard to be certain.
https://www.theatlantic.com/health/archive/2022/04/covid-ba2-omicron-invisible-wave/629708/?utm_source=feed